In November 2013, the AHA in association with the ACC released novel guidelines regarding the management of hyperlipidemia. These guidelines essentially separate management into two broad categories; primary, and secondary prevention.
Primary prevention is separated into patients with LDL-C > 190mg/dL, patients with diabetes mellitus (type I or II) aged 40-75, with the remainder of patients stratified based on their estimated 10 year ASCVD risk.
In a strongly positive move, all patients with a history of ASCVD, defined as a history of MI, stable or unstable angina, any arterial revascularization, stroke, TIA, or peripheral arterial disease of atherosclerotic origin, are recommended to be prescribed a high-intensity statin unless contraindicated or intolerant.
Statins have been categorized into high-, moderate-, and low-intensity based on their predicted percentage reduction in LDL-C. Below is a table outlining these categories and the statins which satisfy each treatment criterion.
| High-intensity | Moderate-intensity | Low-intensity |
| Daily dose lowers LDL–C on average, by approximately ≥50% | Daily dose lowers LDL–C on average, by approximately 30% to <50% | Daily dose lowers LDL–C on average, by <30% |
| Atorvastatin (40)–80mgRosuvastatin 20 (40)mg | Atorvastatin 10 (20)mgRosuvastatin (5) 10mg
Simvastatin 20–40mg Pravastatin 40 (80)mg Lovastatin 40 mg Fluvastatin XL 80 mg Fluvastatin 40 mg bid Pitavastatin 2–4 mg |
Simvastatin 10 mgPravastatin 10–20mg
Lovastatin 20 mg Fluvastatin 20–40 mg Pitavastatin 1 mg |
Below is an outline of the new guideline, summarized in a flow chart.
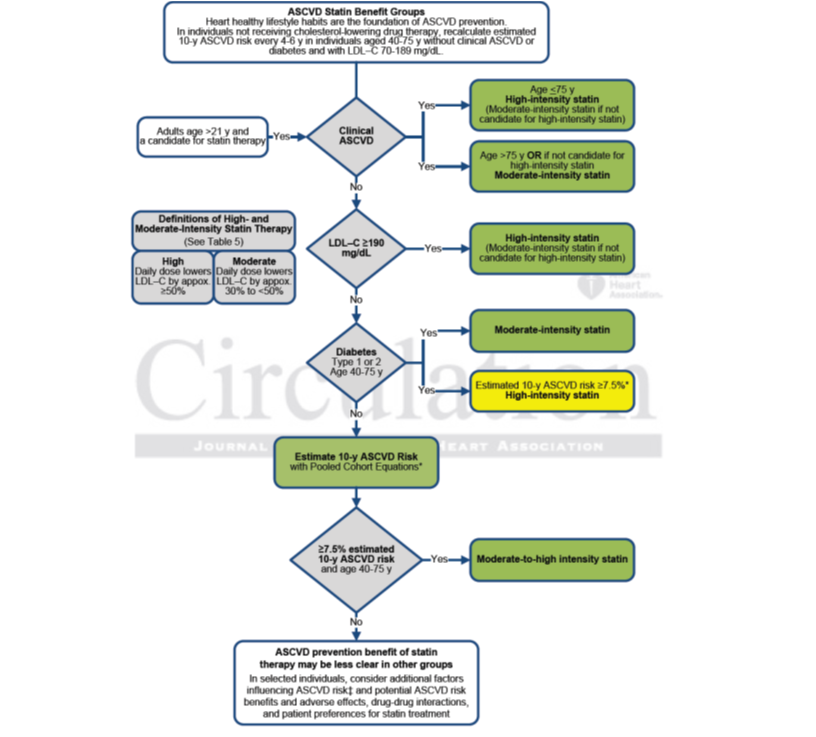
Changes to statin therapy guidelines for risk reduction of atherosclerotic cardiovascular disease (ASCVD)
What does this mean for the way we practice/prescribe?
- Anyone with history of ASCVD should be prescribed the highest tolerable dose of a statin
- Risk stratify patients with normal LDL-C using the excel spreadsheet attached and treat accordingly
- 10 year ASCVD risk 5% < 7.5% are suitable for moderate intensity statin dosage
- No recommendation for primary prevention in patients over 75
- Secondary prevention in patients over 75 should step down from high intensity to moderate intensity.
- LDL-C > 190mg/dL requires high intensity treatment
- Reduced need for LDL-C monitoring
- Reduce statin dosage if LDL-C < 40mg/dL
- Obtain ALT prior to initiation of statin therapy
Difficulties these changes will bring
- No goal orientated therapy (lack of LDL-C monitoring)
- Must continue to advocate diet and exercise
- Other lipid –lowering agents are not recommended under the revised guidelines
- No protocol for patients who experience ASCVD despite maximal statin therapy