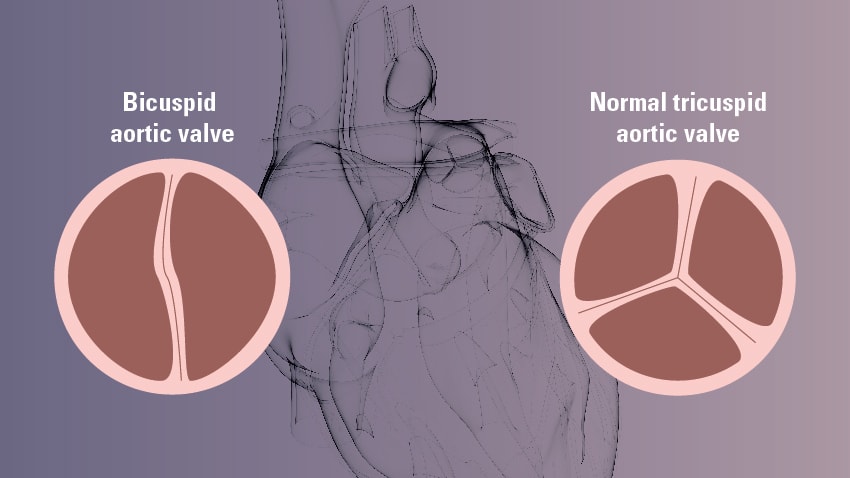
What is a Bicuspid Aortic Valve
This is a common congenital cardiac malformation and it is associated with thoracic ascending aortic aneurysm, dissection, infective endocarditis, sudden death, and progression to aortic stenosis or aortic regurgitation.
It is inherited in a autosomal dominant pattern; however there are also isolated cases, therefore, family members must be screened.
The examination should also look for coarctation of the aorta, and be heard for a heart murmur.
Aortic stenosis tends to occur at a young age, often in the 40s and 50s. If the ascending aorta and aortic root are not well imaged on echocardiography, then a transesophageal echocardiogram should be done. In most cases, I prefer to do the transesophageal echocardiogram for a more complete examination.
Bacterial endocarditis prophylaxis is not needed for dental and surgical procedures unless they have had endocarditis before. However, in a patient with a bicuspid aortic valve with clinical suspicion of endocarditis, a transesophageal echocardiogram should be done.
The ascending aortic imaging should be done to look for an aneurysm and progression of its size. This can be done using CT scan or MRI. Depending on the size of the aneurysm, there are recommendations to avoid intense weight training or exercise.
Surgery is the mainstay of therapy, and the indications for aortic stenosis and aortic regurgitation are defined elsewhere. Repairing the aortic sinuses and replacing the ascending aorta is indicated if the diameter is greater than 5.5 cm. However, if the valve is also going to be replaced or if there is a dissection, then, 5.0 cm is the cutoff. Also, if there is an increase of more than 0.5 cm in 1 year, it indicates progression and replacement is recommended.